Graves’ Disease⁚ An Overview
Graves’ disease is an autoimmune disorder characterized by hyperthyroidism, resulting from excessive production of thyroid hormones by the thyroid gland. This condition leads to various systemic manifestations, significantly impacting the quality of life if left untreated or inadequately managed.
Clinical Presentation
Patients with Graves’ disease often present with a multitude of symptoms, primarily due to the hypermetabolic state induced by excessive thyroid hormone production. Common complaints include weight loss despite increased appetite, palpitations, tremors, heat intolerance, and anxiety. Physical examination may reveal a diffusely enlarged thyroid gland (goiter), and some patients may exhibit exophthalmos or eyelid retraction, leading to a characteristic staring appearance.
In addition to these classic features, some individuals may experience changes in menstrual patterns, fatigue, or muscle weakness. The skin may become thin and fragile, with an increased risk of bruising. Furthermore, some patients may develop onycholysis (separation of the nail from the nail bed) or clubbing of the fingers.
The clinical presentation can vary significantly among affected individuals, ranging from mild to severe. Elderly patients may exhibit fewer obvious signs and symptoms, often leading to a delayed diagnosis. In some cases, patients may present with an isolated finding, such as atrial fibrillation or weight loss, which necessitates further evaluation to determine the underlying cause.
A thorough evaluation of the clinical presentation is crucial in diagnosing Graves’ disease and differentiating it from other causes of hyperthyroidism.
Causes and Risk Factors
Graves’ disease is a multifactorial disorder, influenced by genetic predisposition, environmental factors, and hormonal interactions. Specific genetic variants, female sex, family history, and certain medical conditions contribute to an increased risk of developing the disease.
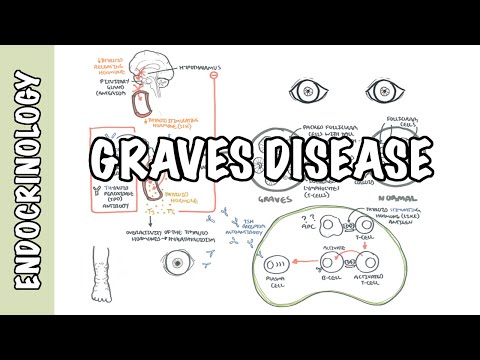
Autoimmune Response
The autoimmune response in Graves’ disease involves a complex interplay between immune cells, thyroid antigens, and autoantibodies. The primary autoantigen is the thyrotropin receptor (TSH-R), which stimulates the thyroid gland to produce thyroid hormones.
In Graves’ disease, TSH receptor antibodies (TRAb) are produced by activated B cells, leading to an exaggerated autoimmune response. These autoantibodies bind to the TSH-R, mimicking the action of thyrotropin-releasing hormone (TRH) and stimulating excessive thyroid hormone production.
The autoimmune response in Graves’ disease also involves other immune cells, including T cells and dendritic cells. Activated T cells produce pro-inflammatory cytokines, which contribute to the inflammatory process and perpetuate the autoimmune response.
The precise mechanisms underlying the autoimmune response in Graves’ disease remain unclear. However, it is evident that a combination of genetic, environmental, and hormonal factors contributes to the development of this complex autoimmune disorder.
A comprehensive understanding of the autoimmune response in Graves’ disease is essential for developing effective therapeutic strategies and improving patient outcomes. Further research is necessary to elucidate the underlying mechanisms and identify novel targets for treatment.
Diagnosis
Diagnosing Graves’ disease involves a combination of clinical evaluation, laboratory tests, and imaging studies to confirm hyperthyroidism and identify characteristic features of the disease, such as goiter and exophthalmos, distinguishing it from other thyroid disorders.
Imaging Studies
Imaging studies play a crucial role in the diagnosis and management of Graves’ disease. The primary imaging modalities used include ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI). Ultrasonography is commonly employed to evaluate thyroid gland size, echotexture, and the presence of nodules or other abnormalities.
CT and MRI scans are useful in assessing the extent of exophthalmos and eyelid retraction, as well as the involvement of surrounding orbital tissues. These imaging studies help identify potential complications, such as optic neuropathy or globe subluxation, which may require surgical intervention.
Radioscintigraphy, particularly with technetium-99m or iodine-123٫ can be utilized to evaluate thyroid function and identify areas of increased uptake. This information can guide treatment decisions٫ including the use of radioactive iodine therapy. Imaging studies should be interpreted in conjunction with clinical findings and laboratory results to ensure accurate diagnosis and effective management of Graves’ disease.
It is essential to consider the benefits and limitations of each imaging modality and tailor the diagnostic approach to individual patient needs, minimizing radiation exposure and optimizing diagnostic accuracy.
Treatment Options
Management of Graves’ disease involves a multimodal approach, including antithyroid medications, radioactive iodine treatment, and surgical intervention. Treatment goals focus on restoring euthyroidism, alleviating symptoms, and preventing long-term complications, thereby improving quality of life.
Radioactive Iodine Treatment
Radioactive iodine (RAI) therapy is a widely employed treatment modality for Graves’ disease, particularly in the United States. This approach involves the oral administration of radioactive iodine-131, which selectively targets and destroys thyroid tissue, thereby reducing thyroid hormone production.
The efficacy of RAI therapy is attributed to the thyroid gland’s unique ability to concentrate iodine, allowing for the delivery of a high dose of radiation directly to the gland. The radioactive iodine is absorbed by the thyroid follicular cells, causing damage to the cells and subsequent reduction in thyroid hormone secretion.
Following RAI therapy, patients typically require lifelong thyroid hormone replacement therapy to maintain euthyroidism. RAI treatment is often preferred over antithyroid medications due to its ability to induce long-term remission and avoid potential side effects associated with prolonged medication use. However, RAI therapy may not be suitable for all patients, particularly those with active Graves’ orbitopathy or large goiters.
A thorough evaluation of the patient’s overall health and medical history is essential to determine the suitability of RAI therapy as a treatment option for Graves’ disease.
Surgical Treatment
Thyroidectomy, or surgical removal of the thyroid gland, is a viable treatment option for patients with Graves’ disease who are not suitable candidates for radioactive iodine therapy or antithyroid medications. Surgery may be indicated for individuals with large goiters, suspected thyroid nodules or cancer, or those with severe Graves’ orbitopathy.
The primary goal of surgical treatment is to remove the thyroid gland, thereby eliminating the source of excessive thyroid hormone production. The procedure typically involves a subtotal or total thyroidectomy, depending on the extent of glandular involvement and the surgeon’s preference.
Surgical complications, such as vocal cord paralysis, hypocalcemia, and postoperative hemorrhage, can occur, albeit infrequently. To minimize these risks, it is essential to select an experienced surgeon with expertise in thyroid surgery. Following thyroidectomy, patients require lifelong thyroid hormone replacement therapy to maintain euthyroidism.
In carefully selected patients, surgical treatment can provide a definitive cure for Graves’ disease, alleviating symptoms and improving overall quality of life. A thorough preoperative evaluation and close postoperative follow-up care are crucial to ensure optimal outcomes.
In conclusion, Graves’ disease is a complex and multifaceted condition that requires comprehensive management to achieve optimal outcomes. A thorough understanding of the underlying pathophysiology and clinical manifestations is essential for early diagnosis and effective treatment.
A multidisciplinary approach, incorporating endocrinologists, surgeons, ophthalmologists, and other specialists, is crucial in managing the various aspects of Graves’ disease. By working together, healthcare providers can develop personalized treatment plans tailored to each patient’s unique needs and circumstances.
Ongoing research and advances in medical technology continue to expand our knowledge of Graves’ disease, enabling the development of novel therapeutic strategies and improved patient care. As our understanding of this condition evolves, it is essential to remain vigilant and adapt our management approaches accordingly.
Ultimately, successful management of Graves’ disease relies on a collaborative effort between patients, healthcare providers, and researchers. By fostering open communication, promoting education, and encouraging continued innovation, we can strive towards improved outcomes and enhanced quality of life for individuals affected by this challenging condition.
I appreciate the emphasis on the variability of symptoms among affected individuals. This highlights the importance of thorough evaluations in diagnosing Graves
This article provides a comprehensive overview of Graves
This article serves as a valuable resource for anyone looking for information on Graves
As an endocrinologist, I found this article to be a useful summary of Graves
The writing style is engaging and easy to follow. I particularly appreciated the use of specific examples to illustrate key points about Graves
The section on clinical presentation is well-written and informative. However, I would have liked to see more discussion on the long-term consequences of untreated Graves